I’d been meaning to write this post for a while, as the doctor’s make adjustment to my high blood pressure (hypertension aka HBP aka HTN) medication, and then I saw it was World Heart Day, September 29th, so I thought, I am going to write it today.
If you were to look at a current picture, I doubt most people would like at it as face value, and think “She has high blood pressure.” If you thought that, you would be wrong. I have had blood pressure for 14 years. Just the other day I was talking to my uncle, and he said, “I didn’t know you had a high blood pressure.”
As I mentioned, I was diagnosed with HBP 14 years ago. It was a very stressful time for me. I was planning a wedding in hometown, and virtually every weekend I spent either going to my hometown or going to see my husband-to-be. That meant either a 2.5 hour drive to my hometown, or a 2.5 drive plus an hour plane ride to see now husband. This is on top of regular life stressors and being in an intensive leadership program for work.
I vividly recall the first time I had an issue with my HBP. I had a horrible headache, and the right side of my face tingled, and I assumed it was my sinuses, as I could get severe sinus headaches and infections. Something about it did not seem right, so I went to urgent care. The wait was long, as it was cold and flu season, and when they examined me, my BP was 150/110. Immediately, the doctors told me I needed to go to the emergency room (ER), especially, since I was having what I now know were neurological symptoms. I drove myself to the ER, and they assess me there, and by this time, by BP is even higher. Did I mention I was living in a place few friends and no family, so of course, being nervous and scared, my BP went even higher.
While in the ER, the doctors and nurses asked me about my family history. Boy, do I have some goodies in my family. For me, it really should be a question of “What don’t you have vs. What do you have?”. All of the adults on my mother’s side and most of the adults on my father’s side have/had HBP, so you would think I would not be surprised to be experiencing BP issues at 27. Well, I was surprised and scared.
The doctor gave me some medication to bring my BP down and sent me home with a BP prescription. Now, normally a person would not get a BP prescription the first time it’s high but over a period of weeks and multiple readings. However, multiple readings typically apply to a gradual increase in an office setting, not an extremely high reading or emergency. I followed-up two weeks later, after diligently taking the new BP meds, and my BP did not improve, not even by a little bit.
The first BP medication failure was my first experience with the difficulties of HBP. It was the first time that I learned that sometimes Black people do not respond to blood pressure medication the way the other races and ethnicities do. Later on in my BP journey, I also learned that some medications in certain medication classes, like lisinopril (ace inhibitor) can cause serious facial and lip swelling (angioedema). Several people in my family on both sides have experienced angioedema, so when doctors try to suggest that for me, I’m like “No, thank you.” The doctor tried another medication, and soon I would move to a new state.
In that new state, and literally every new doctor I saw over the next 8 – 10 years, almost always said the same thing “You’re so young, and at times “You’re a good weight”, I’m surprised you have hypertension. Well, I do, so please give me the same attention and thought you would give to a middle-age man.
A few years into the journey and multiple doctors due to moves, a new issue crops up. I’m seeing my internist for something unrelated, and the nurse goes and gets the doctor after taking my vitals. The doctor comes in and asks me to lay on my left side. He asked “You don’t feel funny, what with your heart rate 130”. I said not really at this moment, but I had been having some issues with being tired and overheated easily. The doctor said, um, yeah, you’re going to the cardiologist. One, because he thought he heard a mitral valve prolapse, and two, for the heart rate. A normal adult at-rest adult heart rate should be between 60 - 100, and at that time, I was consistently over 100.
I went to my first cardiologist, and he did a stress test and had me wear a monitor for 21 days. Let me tell you, the monitor was not fun. I kept forgetting to bring the monitoring phone with me to the bathroom or even just to go to a coworker’s office. I get through the 21 days, and go to the office for a follow-up. The following conversation happened after all pleasantries were exchanged:
Cardiologist: You need to take your medication at night.
Me: Why the switch?
Cardiologist: That’s when the monitor showed you were having the most events and your medication does not last you through the night.
Me: I never received a call from the monitoring company.
Cardiologist: Well, they said they called you.
Me: I’m telling you, in three weeks, not one person called my phone to alert me of an issue. (In my head, shouldn’t the monitoring company reach out to the office, to make sure they have the right contact information). I asked a few more questions I can’t remember.
Cardiologist: Just take the medicine at night.
Me: Okay. (Making a mental note, that this doctor/patient relationship was not going to work).
I immediately asked my internist for a referral to a new cardiologist after the exchange with the first cardiologist. I did not like the fact that I tried to speak up, and was essentially hushed.
Throughout the years, my weight has fluctuated. When I was diagnosed with HBP, I was 27yo, and had a normal BMI, certainly not someone you would expect to be diagnosed with hard-to-control BP. By the end of nursing school and the three years following, I was at my highest weight, probably 165lbs or so. I carry it well, and most people would not think I weighed that. At my highest, my weight put me in the overweight category and probably sometimes, into the obese category. During all of these 14 years of BP issues, very few of my doctors said anything to me about my weight. If anything was said, it was more in the context of watch you eat related to cholesterol, HBP or diabetes. Why didn’t the doctors say anything? Was it because of my health background? Was it because of my age and gender? Was it it because they didn’t want to offend me by mentioning my weight?
I truly do not think doctor’s not mentioning my weight had any real bearing on my current health, because I have the knowledge needed to make change, even if I don’t always practice what I preach. However, what about people who need information about weight and problems that can come from it. More than just saying “You need to lose weight.” I can probably count on one hand doctor’s who gave me actual health information vs. a blanket lose weight.
For nursing school we had to do a community health project and I went to a senior rec center, that primarily served African Americans. Most of the participants had a least one chronic illness, and some did not take their medication at all or take it correctly. Many of the participants said when they were diagnosed with diabetes or HP, that they were not given any information and when they asked about it, doctors and nurses told them to look it up. Those same participants said they were disappointed in the experience and it discouraged them to “do better”. They knew they needed to “do better”, but what is better.
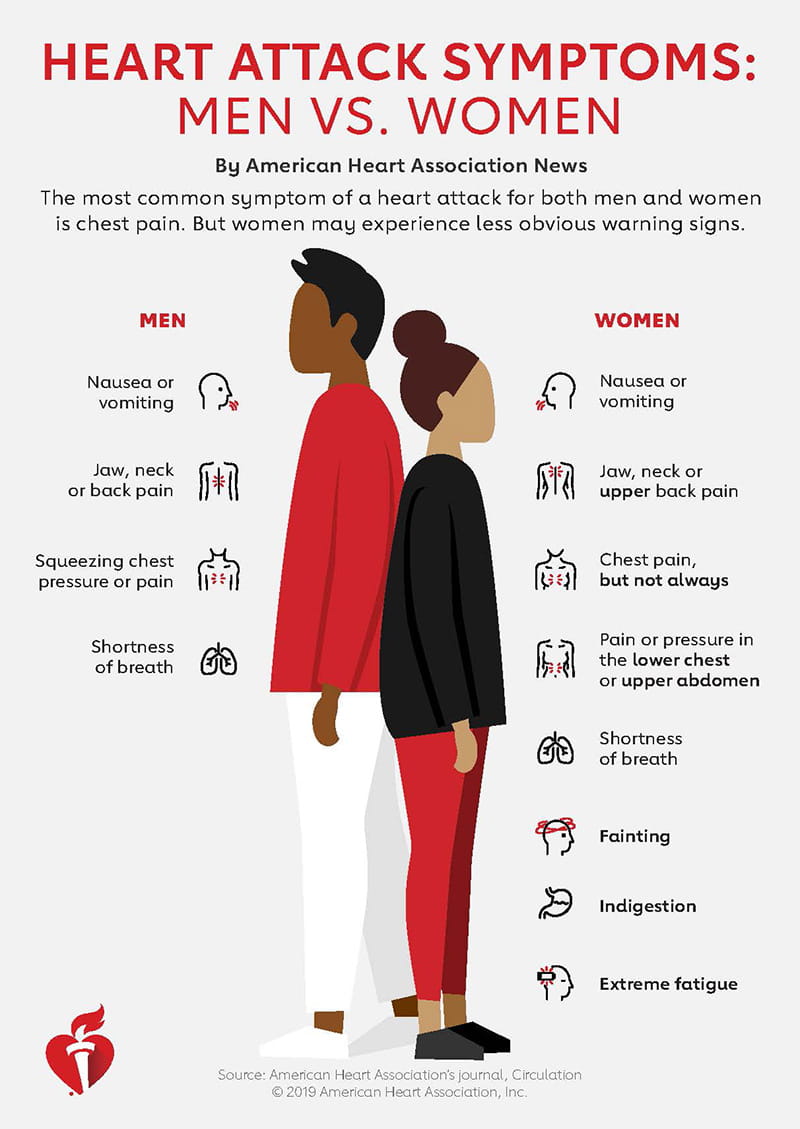
During my presentations, I brought healthy snacks, usually roasted chickpeas, fruit, fresh raw vegetables, and a healthy-ish dessert like sweet potato or black bean brownies. We washed all that healthy goodness down with sparkling or regular water. In addition to snacks, I provided participants with a copy of Leanne Brown’s Eat Well on $4 a Day ($4 is about what someone who receives food gets per day). I also provide stand alone images of the Blood Pressure chart, Stroke Signs, and Heart Attack Signs and Symptoms. If participants are able, we do a Leslie Sansone five-minute booster walk. Some of the participants liked the presentation so much that they asked me to go to their church and do the same presentation. I was happy to do so, and really enjoy doing presentations like that. The participants said they learned how to eat more healthy meals on a budget, how to walk for exercise, and were excited to learn it. It does not mean participants went out and made immediate change or lasting change, but at least they have the knowledge to do so if and, hopefully, when they are ready to do so.
Currently, I am adjusting my medication again. Adjusting my BP medication can be a frustrating experience, from too high to too low, but I am thankful that I have good health insurance, the means to pay for medication, healthier food, and extensive health knowledge. Even 14 years later, I still have trouble sometimes with people listening and like “high blood pressure”. Yes, I do, and please listen, especially, since women can present differently with heart attack symptoms.
Overall, I’m fairly healthy. Lots of small nuisance things, but healthy-ish, nonetheless. I don't always make the best heart-healthy choices, but that is a part of being human. The difference between me and and a lot of other people, is that I'm fortunate to know how to, but as the saying goes "knowing is half the battle." What about the people who do not have insurance or are underinsured, or don’t have easy access to healthy food (food deserts)?I
Advocate, advocate, advocate. If one doctor does not listen, go to another one. We know our bodies.
Stay Safe. Mask Up. Wash Your Hands.
Crafty



]]>